The Medical Zombie

Even zombies stop for a selfie
To listen to most commentators, the medical model lumbers around the mental health landscape like some kind of zombie. It’s dead (or at least out of date), bits of it are always being refuted, we should run screaming when it appears, and if we let it, it will eat our brains, leaving us mindless husks. Even philosophers, who should know better, criticise it in passing without clearly saying what it is, leaving us to guess its evil dimensions from their own prose about what needs changing.

The Medical model is usually defined by contrast with something better
So, this post is going to introduce us to the medical model as it really is. We shall see that it is nothing like what the negative accounts suggest: indeed, many of the “improvements” suggested are actually parts of the model. But, before I say what it is, I need to make clear what it isn’t, which is unfortunately how most commentators treat it.
The Medical Model isn’t a Concept
Think back to when you learned to drive a car (or if you never have, imagine it). The instructor tells you to put your hands here, your feet there, pull this lever in this direction, adjust your feet on these pedals like so, and you’re moving. What you have learned is a procedure, and a procedure is profoundly different from a concept.

A centipede discovering the difference between concepts and procedures
Students learn medicine the way we learn to drive cars. Our examinations, diagnoses and treatments are expressions of these processes. The brain encodes processes so differently from concepts that we give different terms to the memory systems used to store them.
The many kinds of memory
Concepts end up in explicit memory, while procedures are stored in implicit memory. To understand the difference, think back to the car driving example. Your explicit memory could probably have told you what you needed to know about the controls almost immediately. However, it took weeks of practice before your implicit memory could reproduce the necessary movements sufficiently reliably for you to pass a test.
The Medical Model: everything above the water is concept, everything below is procedure. The ship is full of philosophers
The Medical Model is a Skill-Set
Precisely because skills involve procedures, they can be hard to define. The best definition I could find for our purposes turned up in, perhaps unsurprisingly, in a dictionary of business terms

The basic medical skills
After diagnostic skills, which, as I discuss in another blog post, date back to ancient Egypt, practice skills are the oldest component of the medical model. They were first set out in the famous oath, entirely incorrectly attributed to Hippocrates (to give it added force) sometime between the fifth and fourth century BCE.
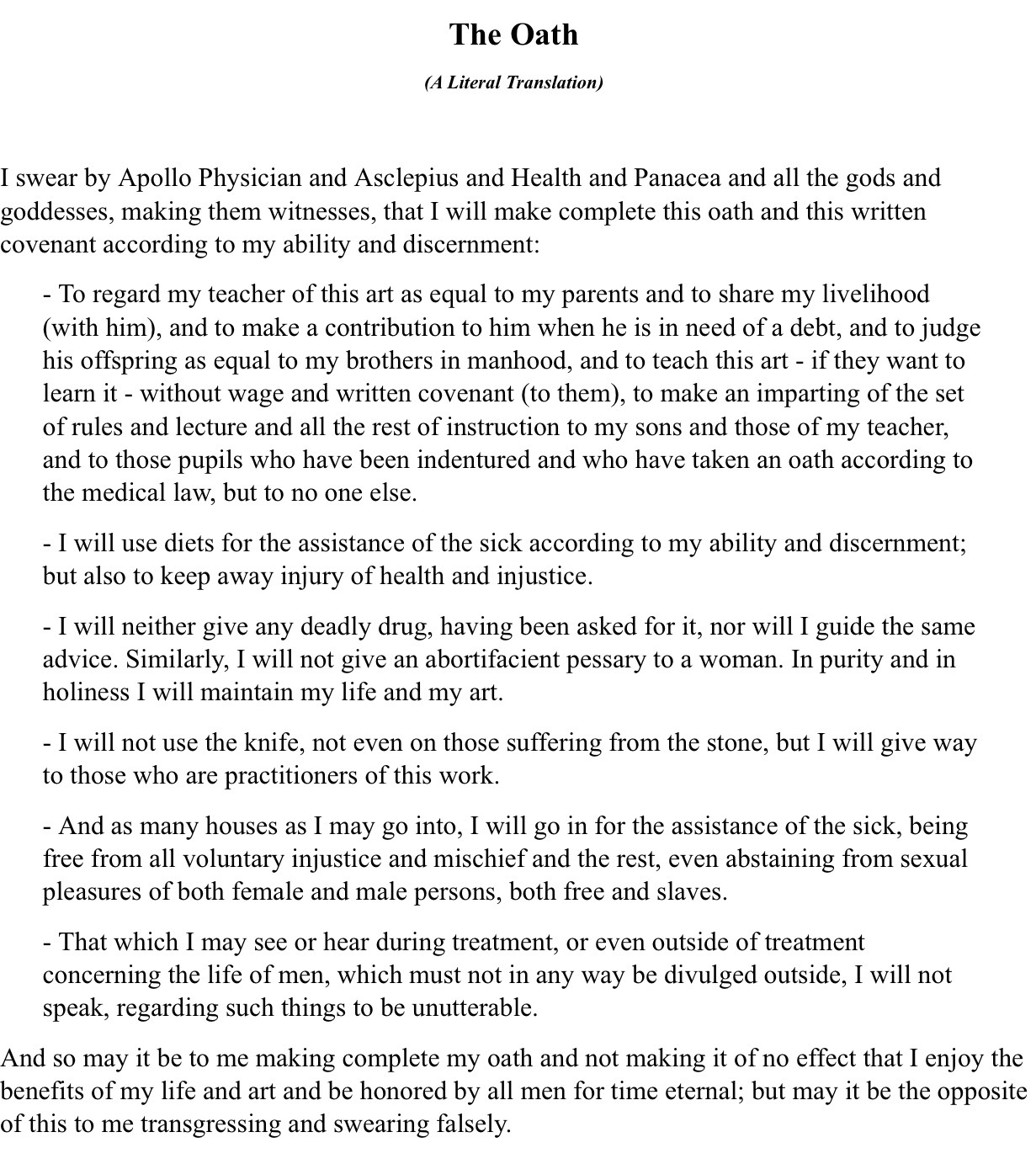
Despite the religious preamble, it’s obvious that we’re looking at a contract. The doctor has committed s/himself to practice in certain specific ways. Ethics are an integral part, but by no means all, of what the Oath covers.
The first paragraph, by far the longest, commits the novice practitioner to support and help maintain his teacher’s practice.
The second promises, to “use diets” reflects the practice of medicine at the time: diet (which actually referred to a combination of recommended food, exercise and sexual activity) was the preferred intervention, to be adjusted according to the patient’s state of health. Ancient Greek medicine had a spectrum between drugs and food so this recommendation did not exclude the use of drugs as part of a therapeutic regimen. “Injustice” here refers to the doctor’s own judgment, so this is a guarantee of quality (which would of course also reflect favourably on the trainer).
The third paragraph says a lot about time-specific ethics (clearly abortifacients were as controversial then as now) but there is a key ethical guarantee: a doctor may not provide what is asked for, if it is harmful. There is also a general requirement for good ethical standards
The fourth paragraph promises not to claim untrained expertise, even if the problem is understood and the need is urgent. Procedural knowledge trumps conceptual knowledge.
The final two paragraphs introduce the ideas of sexual continence and confidentiality in relation to practice.
Updating the language and, mutatis mutandis, the skills’ descriptions, we can now define the basic skill-set of the Medical Model
- When practising, a doctor must deploy s/his best training to s/his best ability
- A doctor must act according to s/his best judgment, to optimise the benefit/harm ratio for the patient.
- A doctor may not act on requests that, in the doctor’s estimation, will hurt s/his patients.
- A doctor will not do things s/he cannot do in practice, even if s/he understands the theory, so will have a good understanding of the limitations of s/his skills.
- A doctor must regulate s/his own behaviour to exclude sexual relationships with patients, ensure confidentiality, and live to high ethical standards.
Having set this out, what is so surprising is the longevity of the model. These principles, with some additions, still remain at the heart of modern medical practice, and remain standards doctors are judged by. Psychiatry is a branch of medicine, and the doctors who practice it, called psychiatrists, must adapt this basic skill-set to the needs of their patients.
Applying the Medical Model’s Skill-Set to Psychiatry
The first rule of adapting the model is that the basic rules haven’t changed. As we no longer live in Ancient Greece, let’s switch to the up-to-date version. The British General Medical Council captures it under four headings.
- Knowledge, skills and performance
- Safety and quality
- Communication partnership & teamwork
- Maintaining trust
We can see that what’s changed since Ancient Greece is mostly under heading 3, where stuff like teamwork and openness sit, consistent with our much more democratic and complex society. These days, consent, not mentioned in the Oath (as the arrangement was commercial, consent was implied), is under 4.
The first thing to notice is how general the model is, regarding the range of knowledge and skills it can use. If a profound knowledge of literature, or the ability to dance superbly, improved our patients’ conditions, then we would be expected to have those skills. However, the model does expect us to be judicious and competent, which are pre-requisites for trust, safety and quality. What does this mean in psychiatry?
Judgment
Not all judgment in medicine is medical
Judgment is possibly the most important of all our medical skills. It is nothing to do with justice, but refers to our ability to make distinctions, so we can do different things to help our patients under different conditions. This is what diagnosis is for, as it has been since Ancient Egypt. I have already blogged about how doctors use diagnosis, and that it may be used differently by other professions, so all I will say here is that diagnoses work as aids to our medical judgment. Provided the judgments reliably lead to ways in which we can help our patients, the Medical Model is entirely agnostic on how true they are. However, the medical ability to diagnose is a procedure, which takes years to acquire. Without that procedural knowledge, which is what leads to treatment choices and prognostic judgments, our understanding of the meaning of diagnosis is incomplete. It is important that psychiatric diagnoses are not completely based in language, as they may refer to conditions that may not be appropriately described linguistically: a label may be the best we can do with words. We can see that, from this perspective, that is nothing reductive or restrictive in the use of diagnosis: if the current one doesn’t fit, we can change it or develop a new one, provided we are competent to do so.
Competence
I guess we can think of competence as a kind of meta-skill: it says how good we are at the skills we claim. What are psychiatrists expected to be competent at?
One thing that makes the Medical Model medical is the centrality of good ethical practice. Like everything else, moral behaviour is something we need to learn, and psychiatric ethics presents us with some of the most challenging problems in all of medicine. Psychiatry therefore explicitly includes lifelong ethical training, which is both elaborately systematised and constantly developing. This is consistent with research findings suggesting psychiatrists are at low risk for malpractice claims, compared to other medical specialities. The good ethical care psychiatrists give their patient arises directly out of the Medical Model’s requirement that ethical skills should not be distinguished from technical skills, combined with recognition of the special ethical problems that psychiatry presents over issues such as consent, meaning a higher level of ethical competence is necessary.
Of course, psychiatrists need technical skills too. These can be broadly divided into
- Assessment skills. These come into play as soon as patients are referred or seen, and are required throughout the psychiatrist’s involvement. Diagnostic skills are probably the best-known of these, but are by no means the only ones, as the psychiatrist must also assess how the diagnosis affects the patient’s life, what the impact of different treatments is likely to be, and how the patient responds. Without all these assessments the psychiatrist cannot know that the benefit/harm ratio (there is no such thing as a risk-free treatment) is correct.
- Treatment skills. A psychiatrist must be capable of selecting the best treatment (which might be none at all); providing, either directly or indirectly, the recommended treatment or the best available, and adjusting or changing it according to the patient’s changing needs.
- Boundary skills. These are rarely mentioned, but are crucial for identifying when the limitations of the psychiatrist’s expertise are reached. An example might be the ability to recognise a psychiatric presentation of a physical disorder.
Notice that the model says nothing about what assessments or treatments should be used: the constraints arise from the requirement for competence, as we are clearly being incompetent if we choose an inappropriate treatment or assessment.
By now, it should be obvious that saying things like “the medical model is excessively biological”, “the medical model puts people in boxes” or their various less flattering synonyms is paying attention to only those parts of the model that are visible as concepts, without also reflecting on the procedures which engage them, without which they cannot properly be understood. It’s time to join the dots.
Working with a Living Fossil

The Medical Model is very old, probably much older than the Oath we used as its starting point. Even that recently, concepts weren’t abstracted the way they are now.

Virtues are descriptors of people, so directly observable, not deduced concepts
What they did understand was tools, and so medicine, of course, has always used tools. We have no problem recognising surgical tools

But here’s a picture of a modern psychiatric tool

which, like any good tool, is subject to redesign and improvement over time. Of course, tools are only one part of a system, which requires skill to use properly

As the image above suggests, we are back to my first blog, which is about how to use our tools to do the job we intend.
Another tool is even more important

The Literature, before it went digital
So, from inside the medical model, diagnosis, the various explanatory models of disorders, treatments, their choices and the evidence which supports them all, are simply tools to be used for the benefit of our patients. This of course does not mean that any idea or action is as good as any other, for without corroborative evidence these are no more than engaging stories or possibilities that cannot offer guidance. It is embedded in empiricism, not theory, and has been so for 3,600 years.
Using Tools Without Training
People who aren’t surgeons generally don’t buy scalpels. Psychologists jealously guard access to many of their tests, for fear of misuse. However, many psychiatric scales, and the core diagnostic manuals, are “out there”, to be used by whoever picks them up. If an untrained person picks up a scalpel, it will still cut, just as an IQ test will provide a score, and a diagnostic manual may offer a diagnosis. But, the outcome can be as different as using amphetamine as a drug of abuse, and as a treatment for ADHD.
What could possibly go wrong?
What are psychiatrists for?
A psychiatrist isn’t there to “give a diagnosis”, though you might get one. They aren’t there to “offer medication”, though that might happen. They aren’t there to promote a “biological model” however you conceive it, though they may offer one as an explanation. A psychiatrist is there to do the same as any doctor since as far back as history can remember: use the medical model for your benefit. We have now seen that is honestly and fearlessly exercising their skills and knowledge on your behalf, if necessary in collaboration with others, and without ideological limitation. It might be incredibly old, but I don’t think it’s reached its sell-by date yet.
