The other day I was reading a blog post by a psychiatrist who I greatly respect. Her post was about how worthy, dreary and unexciting she found modern neuroscience, and how it had failed to live up to its clinical promises, compared to more psychosocial approaches of understanding mental health. However, she also said this.
I would really like to hear more how we can link up a little more across the multidisciplinary divide – and try to understand the interactions between the person, their environment and their brain.
This post is my attempt to say a little more about how I see those links developing, and why, far from being drearily “mindless”, they represent a massive intellectual challenge to clinical psychiatry (and psychology), which we have not begun to address. This challenge may be stated in three words, which make up my first heading.
The Identity Hypothesis
The identity hypothesis is for cognitive neuroscience what the “efficient market hypothesis” is for economics, an unproven assumption which acts as a conceptual foundation for the discipline. It claims that states of mind are also states of brain. Most people these days know the hypothesis, even if they don’t know its name, but tend to say “Yeah, OK” and carry on as before. To show how big a mistake this is, let’s start with an analogy.

This is, of course, the famous image which can be interpreted either as an old woman in profile, or as a young woman turned three-quarters away. It follows that every feature of the old woman is also a feature of the young woman, so here we have not just an identity hypothesis, but a truly dual identity. Despite this, we cannot see both images simultaneously, even though we can readily choose which image to observe. This is true even if we try to focus down on the individual features which are key to the transformation.
Both the optical illusions, and our inability to see past them, provides valuable information about how our visual understanding of the world is processed, including information about when and how much the apparent certainty provided by it may be trusted. This diagram, courtesy of Richard Gregory, shows how much of our visual reality arises from internal processing

What we are doing when we look at a cocktail glass
Our “old-young lady” illusion demonstrates just how powerful that hypothesis generator is. Once we have decided, say, that we have seen an ear, rather than an eye, our visual hypothesis generator imposes such a large confirmatory bias as we process other forms in the image that we must perforce encode the whole as a young woman, despite knowing things can be otherwise.
We may also be affected by illusions of identity, as wittily demonstrated in this painting by Magritte
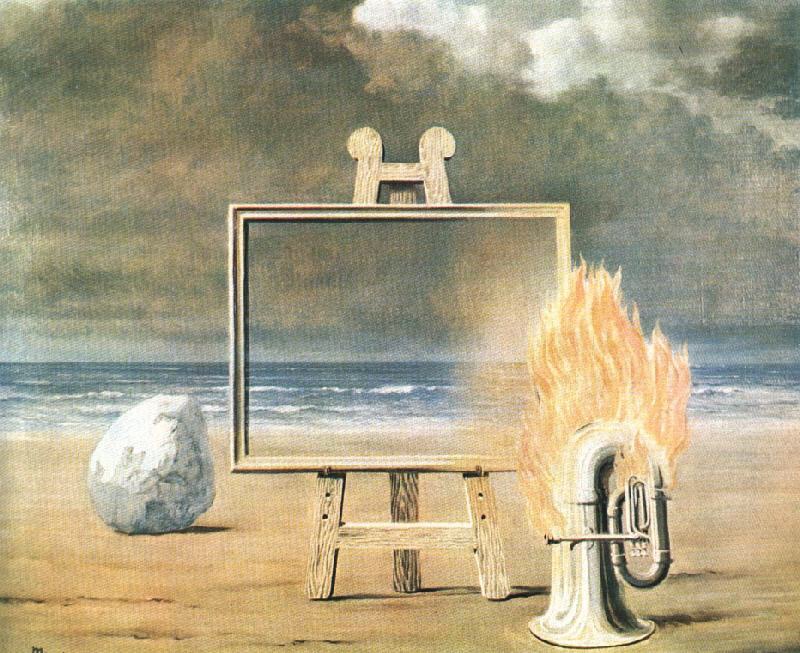
We are confronted by a painting of the sea, set on an easel in front of, and depicting, the same sea, in the same moment that is recorded in the painting. Most viewers will feel this is uncanny. What is happening is that the painting, through our long familiarity with pictures, is creating an illusion that the background sea is more real than that in the frame, when the frame, the frame’s contents and the background, arise simply from cunningly contrived reflections of light on painted canvas: there is no sea. The flaming tuba illustrates the greatest power of the illusion of identity: it can make the impossible seem possible, as we now see so often in our films

An impossible duel brought to us by computer generated imagery
We need to unpack the identity hypothesis a little, to appreciate what it is really saying.
The Identity Hypothesis
We are talking about all our possible states of mind: in symbols ∀{Μ}
We are also talking about a set of possible brain states {Bi}
We go on to claim that, for all our states of mind, there will be corresponding brain states, and that each of those brain states will be reflected in the equivalent state of mind.
In symbols we write ∀M(Mi ≡ Bi)
Note that this allows the existence of a complementary set of brain states {Bj} that do not contribute to states of mind. That’s needed to cover things like coma, the brain’s internal housekeeping etc.
∀M(Mi ≡ Bi) allows us to predict any state of mind from its corresponding brain state (assuming we can identify it), and vice versa.
However, we also know no two brains are identical, and as brains develop and senesce, an individual brain’s function will also vary through the life cycle, as well as being affected by e.g., illness. We also need to include this brain variability {V}.
In symbols, we write ∀M(Mi ≡ Bi | Vi)
Which means, “states of mind and brain states may be used to predict each other, conditional upon relevant brain functioning”
Here is a visual representation of all three components of the identity hypothesis.
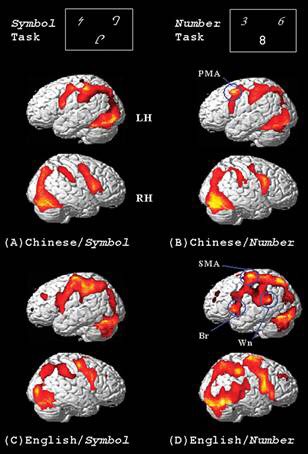
The image shows brain activity related to two different tasks, performed by two different groups of people. We can see that tasks involving symbols and those involving numbers involve different (albeit overlapping) brain geographies. This is Mi ≡ Bi. However, which geographies are involved also depends on which language the brain employs (Vi). This doesn’t prove the hypothesis: we have only tested it in one direction, as we cannot trigger brain states with sufficient accuracy, and it only exemplifies one set of tasks and conditions. But, to date, no exception has been found.
Thinking about the Identity Hypothesis from Inside the Box
Read books of philosophy and one could easily believe that thinking happens in an unrestricted and infinite mental space, where thought can freely move without obstacles or pitfalls. However, if we think with our brains, then this is nonsense. Optical illusions teach us that the brain struggles with dual identity in the visual world, and there is good reason to think similar limitations hold more generally.
At present, we write about states of mind using language, while states of brain are described using mathematics (either visually or algebraically expressed). We have already seen that these all use different brain systems. Are there limits to how we can put them together? While we don’t fully know the answer, we do know that different languages support learning mathematics to different extents, and we are also aware of mathematical objects which exist, but cannot be denoted in language, such as the square root of -1. There is also an everyday example, which is particularly telling as it involves our emotions: music.
A musical challenge to psychosocial formulation
I love opera. Richard Wagner (who also helped to prove that talent is independent of moral rectitude) described it as “Music Drama.” These days, when we go to a performance, we are assisted by “surtitles”: translations of the lines into our local vernacular displayed above the stage. However, even before surtitles, people who did not speak the opera’s language could still follow most of the development of the plot, from a combination of the action on stage and the music that was playing. In ballet, opera’s close relative, we follow the story simply from music and dance. From this, as well as musical forms such as tone poems, we know that music can tell a story. Furthermore, the story is being told through our emotions.
Psychologists argue that music bridges language and emotion, eliciting the latter through temporal information common to language and music, so suggesting an innate dimension of emotional encoding.
This encoding can be visualised as a brain state
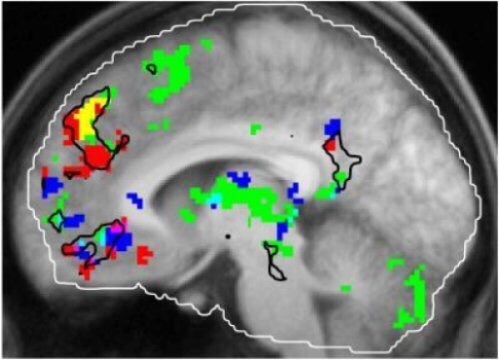
When people are familiar with a tune, their brains show increased activity in the regions shaded in green in this fMRI image. Red areas respond to salient autobiographical memories, and blue areas respond to tunes that a person enjoys. The brain region known as the dorsal medial prefrontal cortex responds both to familiarity and autobiographical associations (yellow).
A lifelong music buff, Janata had earlier created a model for “mapping” the tones of a piece of music as it moves from chord to chord and into and out of major and minor keys. By making tonal maps of each musical excerpt and comparing them to their corresponding brain scans, he discovered that the brain was tracking these tonal progressions in the same region as it was experiencing the memories: in the dorsal part of the medial pre-frontal cortex, as well as in regions immediately adjacent to it. And in this case, too, the stronger the autobiographical memory, the greater the “tracking” activity.
“What’s cool about this is that one of the main parts of the brain that’s tracking the music is the same part of the brain that’s responding overall to how autobiographically salient the music is,” Janata (the researcher) said.
In this particular case Mi is the state of mind associated with familiar, emotionally charged music, while the the dorsomedial prefrontal cortex is necessary for Bi. This state of mind is pretty universal, and we can recognise its commonality, mutatis mutandis, across individual memories and pieces of music. However, like the rest of us, the researcher ends up with an ungainly mix of memory, music and emotion to describe something we experience as a single state of mind, without fragmentation being apparent in Bi either.
Now, let’s think back to our old-young woman. Every feature was both a part of the young and the old image: a perfect correspondence. What we have expressed here is Mijk ≡ Bi, where the subscripts ijk refer to the combination of memory, music and emotion that is equivalent to Bi. Notice, however, that there is nothing in the language-based definitions of music, memory and emotion to link them (in symbols D(i,j,k,) ≉ Mijk). We can therefore write, for our everyday definitions, (Di ⊥ Dj ⊥ Dk) | Bi, where ⊥ signals conditional independence, and |, as previously, denotes conditionality. It is obvious that, simply staring at the images (Bi) without knowing the mental states being explored (Mijk) wouldn’t be enough to deduce the latter. Our demonstration of the independence of D(i,j,k) from each other, conditional on Bi, shows that we also have no way of reasoning from how we normally understand these states to the idea that they are conjointly instantiated in a single brain state, as independence means “no link is as likely as any link.” So, we may not even put the three together, and would be able to argue with anyone who does. What we have shown is that our linguistic and brain based formulations are as separated as our young and old female images; without separate knowledge that they correspond, we cannot combine them, even though we can move smoothly enough between them once we have ascertained their joint existence.
Having chopped all the logic we need, we can now set out our musical challenge
- In the absence of brain–based evidence, no psychosocial formulation, no matter how reasonable, and even if the patient agrees, can be assumed to describe how the patient has encoded the formulation’s topics in the brain.
- If we are formulating a patient’s emotional trajectory, then a musical formulation, validated by the patient’s confirmation of the experiences elicited by the music, is likely to have a closer connection with the brain than a linguistic one, as the additional layer of linguistic definition, and requirement for reason, is absent.
The purpose of this challenge is not to suggest we should all start humming to our patients, and music therapy is not the topic of this post. Instead, what this does is to show that the constraints imposed on psychosocial formulations by the identity hypothesis, when combined with our cognitive limitations, undermines our received wisdom that any psychosocial formulation, however well constructed, and even if checked with the patient, is the best way of understanding our patients. The next section thinks about how this happens.
My Tuba is on Fire! The spurious rationality of the psychosocial formulation
Most psychiatrists, even religious ones, accept the identity hypothesis in their practice. In fact, it does not deny spirituality per se, as it simply asserts that, like all other states of mind, a spiritual experience will have an idenfiable brain state associated with it. However, though there are a few exceptions, psychiatrists make an additional assumption that, even if it occurs at all, parapsychological influence on the brain is too rare and/or faint to account for the hallucinations and delusions presenting in their clinics.

This version of the identity hypothesis asserts that brain states cause (using Aristotelian terminology, are the efficient cause of) states of mind. Attempts to help people with mental illness by assuming otherwise tend to end badly.
It’s worth listing what follows from this version of the identity hypothesis.
- The brain is connected to the world (through its sensory and motor nervous systems) and interacts with it
- Accessible states of mind are how it communicates to us (and partly also to itself)
- Mental health business is changing certain brain states, recognised through states of mind
- If it is to be effective, any treatment, be it physical, psychological or social, must improve the brain state causing the problem
So, any understanding of our patients must be able to predict how their brain states will respond to the intervention we choose, even if that brain state is measured through a corresponding state of mind. The previous section showed how our psychosocial formulations could not be trusted to make the necessary link. This section examines how they can nonetheless trap us in committing to them.
Meaning and its imitators
Consider this list of words
furiously sleep colourless ideas green
They appear pretty random, don’t they? However, if we rearrange them we get
Colourless green ideas sleep furiously.
This famous sentence was coined by Norman Chomsky in 1957, to illustrate how meaning arises from syntactic structure
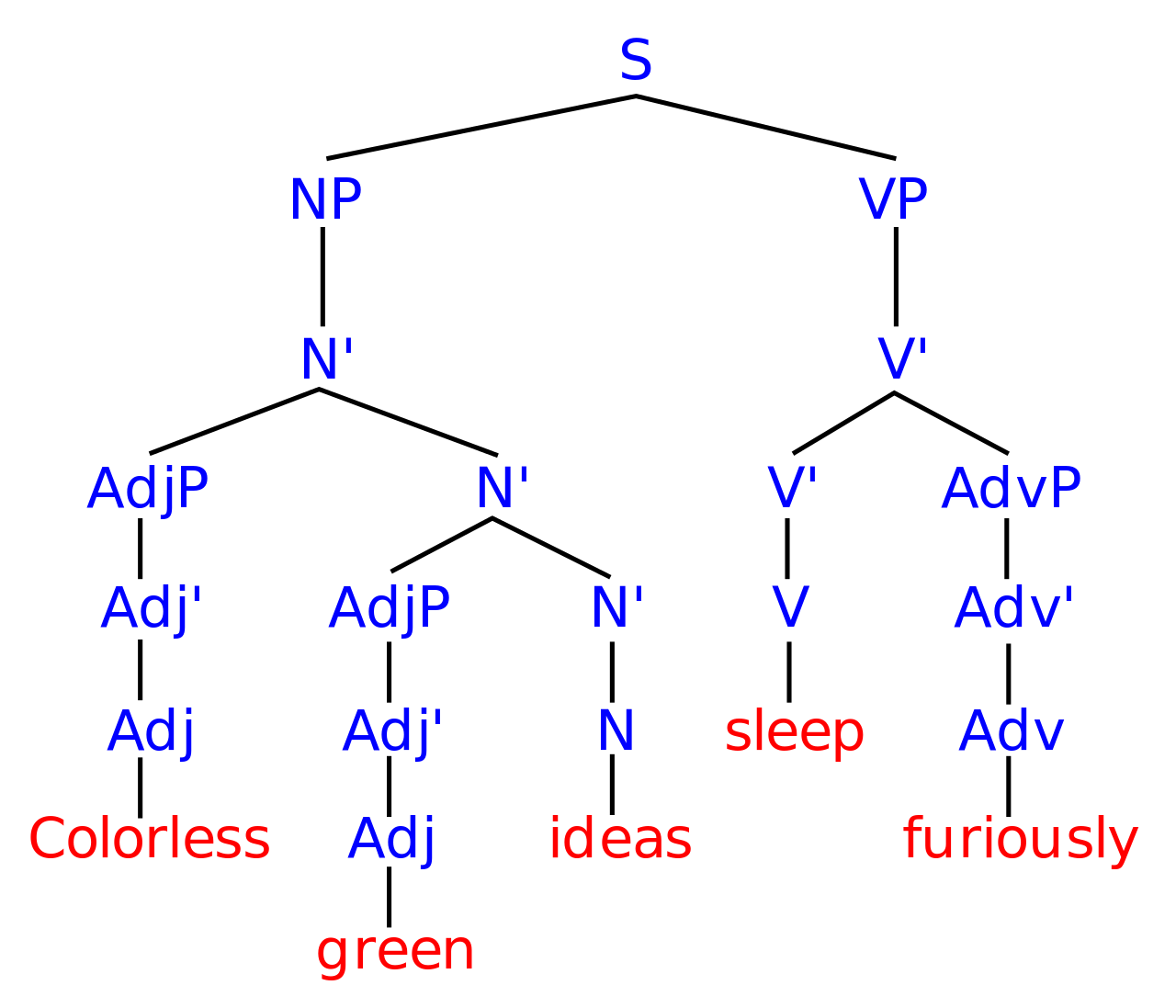
Syntactic structure giving meaning to a set of otherwise random words

Jean Arp with a piece of his work
While Chomsky was trying to create an illusion of meaning, and Paul Eluard was trying to capture the thought and work of an abstract artist, both independently discovered a similar technique; to arrange words so that their juxtaposition suggests meaning, even though their individual definitions did not. The discovery that symbols actually derived their meaning from connection to other symbols, rather than what they symbolise, was actually made by Ferdinand Saussure, Chomsky’s great predecessor. If we look back to our Matisse, we can see exactly the same technique being used on our visual sensorium. It works because both language and vision rely on feature detection to construct the reality we observe. Chomsky’s sentence is a verbal analogue of Matisse’s burning tuba: the plausible juxtaposition of Matisse’s images and Chomsky’s words are both perceived as meaningful, even though the individual interpretations of each word or form warn us they should not be combined.
The hidden surreality of psychosocial formulation
Both psychiatry and psychology have broadly similar approaches to formulation. Summarising greatly, they are purposeful documentary accounts of the patient’s condition, which specifically include and link to relevant theory, and thereby provide both understanding and guidance to appropriate remedial action.
This statement is part of the psychology guidance
However, psychological formulation starts from the assumption that ‘at some level it all makes sense’ (Butler, 1998, p.2). From this perspective, mood swings, hearing voices, having unusual beliefs and so on can all be understood as psychological reactions to current and past life experiences and events, in the same way as more common difficulties such as anxiety and low mood.
In terms of the identity hypothesis, the authors are asserting that the states of mind associated with psychosis, {Mp}, should not be understood differently from ordinary mental responses to the environment {M}, so we should write Mpi ≡ Bi ≡ Mi. Because equivalence is commutative, we are also asserting that Mpi ≡ Mi, which is obvious nonsense. Why then is the claim so plausible? First, it uses descriptors of psychosis (hearing voices, unusual beliefs etc) {D(p)} instead of the set of psychotic experiences itself {Mp}. As our musical challenge showed, substituting one for the other leads to different conclusions. It also proposes an entireIy different cause for states of mind; “psychological reactions”. To the identity hypothesis, a psychological reaction is simply another state of mind, reflecting a brain process intermediate between two others. It is therefore no more than a subset of either {Mp} or {Mi}. However, its linguistic position within the verb part of its sentence biases us to believe, impossibly, that something non-physical can be an efficient cause. The truth being presented here is the same as that found in Eluard, Arp or Matisse, not everyday reality.
Why we should never confuse life with literature
At the same time, a major criticism of psychiatry at present is that there is a reductionist overemphasis on diagnosis and biology. Psychological care is sometimes seen as the domain of psychologists, with psychiatrists’ roles becoming increasingly confined to prescribing and managing psychiatric problems that have a physical basis. A less limited view of what it is to be a good psychiatrist depends on psychiatrists being able to offer psychologically minded care. Formulation is a key part of this, and of making psychiatric practice more therapeutic.
It’s clear that a “reductionist…overemphasis on biology” is not consistent with an appreciation of the significance of the identity hypothesis. Our current understanding of brain states requires more biology, not less. The implied claim that the identity hypothesis’ biological approach impedes psychological care is equally wrong. Think back to our old-young woman. We can use either our “old” or “young” understanding of her features, provided we know either denotes the same feature set. If we know that our psychological descriptions match brain states, there is nothing to stop us using them. In the absence of knowledge about the corresponding brain state, knowing that a treatment is effective for a condition implies it can alter brain states in the desired direction. So, far from being problematic, the identity hypothesis predisposes us to adopt an evidence-based approach to the choice and delivery of psychological treatments. The fact that the same arguments are entirely general, so can also be applied to the equally sketchy theories surrounding drug or social therapies, is an added bonus, as it gives a theoretical base for using physical, psychological and social therapies conjointly, as well as separately.
By now, it should be clear that there is something seriously wrong with how we think about our mental health, if we accept the identity hypothesis. The cognitive errors we’ve explored explain how they have arisen; it’s time to move on to thinking about why.
The Religious Interpretation of the Biopsychosocial Model
This model underpins both sets of guidance we’ve just critiqued. It is usually ascribed to George Engel’s papers in 1977-80, though it was actually developed in the early 20th century by Adolf Meyer. The identity hypothesis has no problem with it, as biology, psychology and sociology simply describe different classes of influence on brain states (though in sociology, the brains are studied en masse, and their states therefore assumed to be averaged, rather than proceeding brain by brain). Despite the comments quoted above, this is not reductionistic, as it does not preclude patterns which are only apparent when interactions are considered, as the picture below illustrates.

Dots interacting to make an image. Now imagine them as brain states

Where the Biopsychosocial Model happens

This kind of reasoning has a venerable (and venerated) history, as it was used by St Thomas Aquinas to describe how body and soul combined to create human beings

There are two requisites for one thing to be the substantial form of another. One requisite is that the form be the principle of substantial being to that whereof it is the form: I do not mean the effective, but the formal principle, whereby a thing is and is denominated ‘being.’* The second requisite is that the form and matter should unite in one ‘being’; namely, in that being wherein the substance so composed subsists.

every aspect of our human existence is simultaneously biological, personal, social and historical
However, the problem with all metaphysical accounts is that there is no way for the non-physical to influence the physical, which gets us here
This approach thus creates an impassable causal barrier between states of mind (which is where we find the issues we subject to formulation) and brain states (which is what we want to change). Unfortunately, it follows from our previous arguments that, without the possibility of such a link, we will not be able to see past whatever illusion the language of our formulation puts before us.
An Unsatisfactory Solution, but the best we’ve currently got: diagnosis as Sancho Panza.

Formulation and diagnosis exploring the unknown
Compared to the intellectual sophistication of generating a formulation, assigning a diagnosis seems almost pathetically simple: elicit a set of symptoms and/or signs, match them to a standard template, and offf you go. However, if the diagnosis has been well established, the list has been standardised across lots of brains in lots of states of mind. Let’s now think back to our full version of the identity hypothesis. It was “every state of mind M can be mapped to a corresponding brain state B, conditional upon relevant brain functioning V“. In symbols we wrote this as ∀M(Mi ≡ Bi | Vi). Provided the validity samples for the diagnosis were sufficiently large, all relevant states of mind and brain states will have been captured, even if we don’t know precisely what they are. That means our diagnosis is pointing squarely at relevant brain functioning Vi. Better still, if we make the not unreasonable assumption that Mi ≡ Bi would be normal in the absence of Vi, then we can restrict our attention to Vi, rather than the much more challenging (because it’s so much larger and more variable) set of Bi. Unfortunately, in mental health we still mostly have to infer Vi through the set of symptoms and signs we observe, summarised as a diagnosis. Furthermore, the symptoms and signs we usually use to make a diagnosis will very often be a subset of the complete list of criteria. In symbols, we write this as follows
Where
- {} indicate sets
- () indicate terms to be read together
- s is the symptoms and/or signs we observe
- S is the full set of diagnostic criteria
- Δ is the diagnosis
- V is brain functioning
- ⊆ means the former term is a subset or equal to the latter term
- X ⊃ Y means “If X then Y”
- i indicates correspondence
{s ⊆ S} ⊃ (Δi ⊃ Vi)
Which shows why things can go downhill. First, because of {s ⊆ S}, we should re-write it as
{s ⊆ S} ⊃ (Δi ⊃ {V₁…N})
Where {V₁…N} are the brain states associated with each possible subset of S. We can’t even be sure if our initially proposed set of criteria is complete! We can see the practical effects of this when we come to treatment; we often have to sift through several (including some combinations) before we get one that can modify Vi. There is, however, a ray of sunshine. Because {s₁…N} overlap each other, the identity hypothesis predicts that {V₁…N} will overlap too, as the state of mind associated with any elementary symptom will associate with a specific brain state, even if we’re not quite sure what an elementary symptom is. This is consistent with our real life observations that alternative treatments do resemble each other. So, we can think of even imperfect diagnosis as a kind of lens, focusing our attention on the treatments most likely to work.
Secondly, because we’re only talking about one-way inferences, this can be re-written as
~{s ⊆ S} ⋁ (~Δi ⋁ {V₁…N})
Where “~” means “not” and “⋁” means “and/or”.
In English, this is the almost incomprehensible “either there isn’t a set of symptoms, which may either be a subset or the full set of diagnostic criteria, and/or there either isn’t a diagnosis and/or a corresponding set of brain states.” But, what it means is that the set of brain states may exist without the diagnosis, and either the diagnosis or the brain states might exist without the symptoms. Though theoretically awful, this can be managed empirically by validity studies. Let’s use a simple example to see how this works.

Using the same notation, what he’s discovered is
Rub sticks ⊃ stick fire
Let’s imagine he keeps experimenting, until he can make fire reliably. He will probably deduce
Rub sticks & long time & stick dry ⊃ stick fire
However, because he can do it reliably, he can also say (provided he ignores the time dimension)
Stick fire ⊃ rub sticks & long time & stick dry
Because he also knows that, while he’s seen fires caused by volcanoes and lighting, they’re not happening nearby right now (or the story would have a tragic ending).
Putting these together, he arrives at
Stick fire ≡ rub sticks | sticks dry, long time.
Notice this is conditional predictive validity: he knows that spending a long time rubbing sticks together will result in fire, and if he sees a fire of sticks it’ll be because someone else has done the same, provided the circumstances are similar. Obviously, the process of validating diagnosis is much more complicated, and the conditional assumptions harder to verify. But, the basic principles, to move from “if then” to “equivalent to”, under specified conditions, is the same. However, the chained implications that currently link diagnosis to its causal brain conditions, and their likely multiplicity, make validation prolonged, demanding and difficult to achieve.
We can think of diagnosis under these conditions as being rather like Sancho Panza to formulation’s Don Quixote. It’s more limited, has smaller ambitions, and its reliability (and therefore validity) can sometimes be suspect. However, it makes up for all this by offering a route to the real world, which is formulation’s Achilles heel.
The Promise of Cognitive Neuroscience
The promise of cognitive neuroscience can be expressed quite simply: it offers to directly represent both brain states Bi and their associated brain variability Vi, thus drastically shortening the chain of implication and its associated uncertainty. This would allow us to create the conjoint psychological and neurological space we need to make best use of the identity hypothesis.
If we set aside our religious interpretation of the biopsychosocial model, and accept that, at the very least, we can’t confidently connect a formulation to reality without a brain state, then cognitive neuroscience has already started to prune unrealistic formulations.
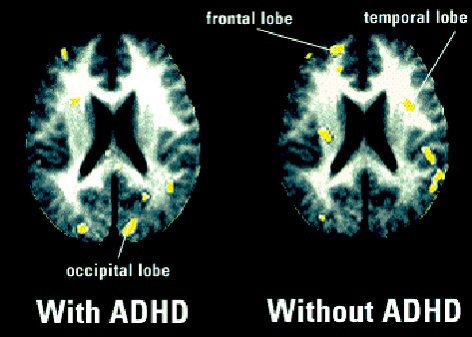
In men who had ADHD, PET scans showed that they processed a memory task in visual areas in the occipital lobe of the brain, as indicated by the yellow spots in the left image. Non-ADHD men used the temporal and frontal lobes, shown at right (ABCNEWS.com)
We can also show that effective psychological treatments target brain states thought to generate psychiatric diagnoses, and aren’t just soothing talk. Here’s a theory of brain states Vi relating to depression
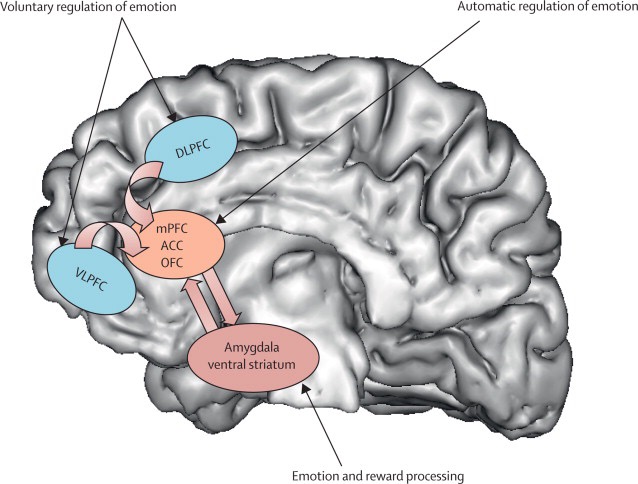
Neural regions involving in voluntary and automatic regulation of emotion, and emotion and reward processing shown in the human brain OFC: orbitofrontal cortex, ACC: anterior cingulate cortex, VLPFC: ventrolateral prefrontal cortex, mPFC: medial prefrontal cortex, DLPFC: dorsolateral prefrontal cortex. source: Kupfer et al., 2012
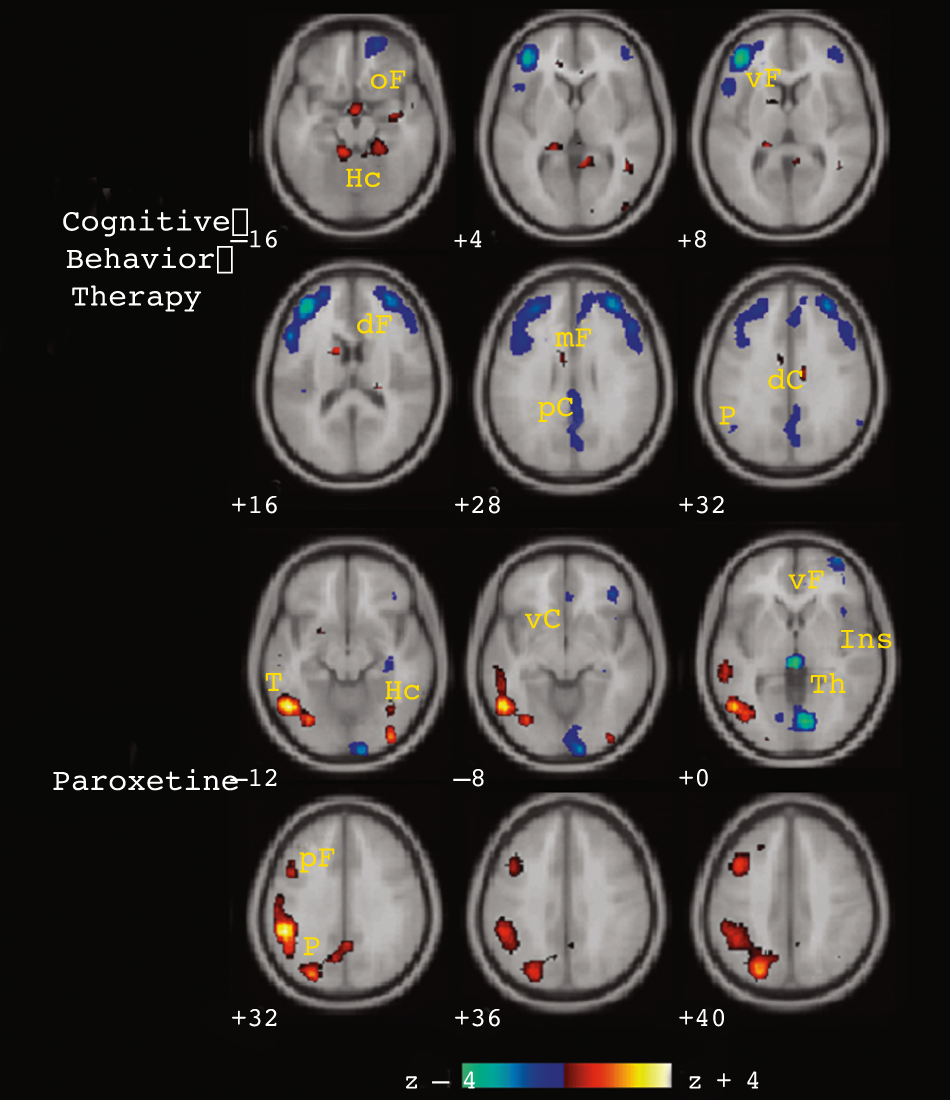
Changes in regional glucose metabolism(fluorine-18–labeled deoxyglucose positron emission tomography) in cognitivebehavior therapy (CBT) responders (top) and paroxetine responders (bottom)following treatment. Metabolic increases are shown in orange and decreasesin blue. Frontal and parietal decreases and hippocampal increases are seenwith CBT response. The reverse pattern is seen with paroxetine. Common toboth treatments are decreases in ventral lateral prefrontal cortex. Additionalunique changes are seen with each: increases in anterior cingulate and decreasesin medial frontal, orbital frontal, and posterior cingulate with CBT and increasesin brainstem and cerebellum and decreases in ventral subgenual cingulate,anterior insula, and thalamus with paroxetine. oF Indicates orbital frontalBrodmann area (BA) 11; vF, ventral prefrontal BA 47; Hc, hippocampus; dF,dorsolateral prefrontal BA 9/46; mF, medial frontal BA 10; pC, posterior cingulateBA 23/31; P, inferior parietal BA 40; T, inferior temporal BA 20; vC, subgenualcingulate BA 25; ins, anterior insula; and Th, thalamus. Slice location isin millimeters relative to anterior commissure. Numbers are BA designations. Goldapple et al 2004
As glucose is the fuel the brain uses, glucose metabolism is a marker of brain activity. We can see that the frontal areas of the brain identified in our model have become less active following Cognitive Behaviour Therapy (CBT). As frontal brain activity is largely inhibitory, it suggests that CBT might lead to less inhibition of our innate emotion regulation systems. However, the involvement of other areas as well, and the very different pattern showed by an equally effective antidepressant, suggests that our current model Vi is overly simplistic, and needs updating. Applying the identity hypothesis means that we might also want to look for additional symptoms and signs of depression, which we know, from our previous analysis, might have no conceptual relationship with those we currently use, and so could not be guessed at otherwise. This is using constant comparison of our psychological and neurological maps to improve both, rather like this

The Cave Brothers encouraging each other to go faster
- We will only find cognitive neuroscience helpful if we learn to understand the identity hypothesis correctly. As we have seen, that may not be easy, or even acceptable for some.
- Cognitive neuroscience has the potential to significantly improve our diagnoses, which are what connects our formulations with the bit of reality we need to change, if our patients are to get better.
- Cognitive neuroscience (used with the identity hypothesis) enables us to require that any formulation is consistent with cognitive neuroscience studies.
- In the event of an inconsistency between a formulation and a cognitive neuroscience study, the onus is on the formulator to demonstrate errors in the study, irrespective of the plausibility of the formulation.
- Including neuroscience in our formulations helps us define what we do not know about our patients. The linguistic structure of psychosocial formulations makes them bad at this.
- Just as with diagnosis, cognitive neuroscience offers the opportunity to identify potential treatments which could not otherwise have been imagined.
It is now generally accepted that there have been no major clinical advances in treatment for a generation. While this can be regarded as a failure of the promise of neuroscience, an alternative could be that our religious interpretation of the biopsychosocial model has prevented us from generating good clinical hypotheses that neuroscience could test.
In the blog that inspired this response, my colleague commented that she
wanted to be a doctor who listened, thought carefully about the options, discussed them, and then tried to help using every avenue available.
Unfortunately, given the current state of our knowledge, “trying to help” (especially without guidelines) can involve an awful lot of false alleys. It would be great if this could be improved, and maybe thinking differently about neuroscience in clinical practice, and the identity hypothesis, might help. I agree with her that there is certainly still lots to think about.
