The debate over whether formulation or diagnosis best captures psychiatric disorder waxes and wanes, but never goes away. In the world of those who spend huge sums (think six and even seven figure sums) on perfect music reproduction, a very similar debate occurs, only this time the opponents are those who favour digital, versus those who prefer analogue reproduction. In fact, the analogue-digital debate among audiophiles can teach us a lot about our own argument, and why we aren’t likely to resolve it anytime soon.
Just like psychiatry, Hi-Fi has two approaches to evaluate perfection. One involves lots of gadgetry, which can say how similar the sound that comes out of the system is to the sound that goes in. This is the science. The other is our ears, and the response we get to hearing the reproduction: of course, we usually don’t get to hear the original sound that was recorded, so we have to imagine it instead. You can guess what happens: the reproduction the machinery reports as best isn’t always what our ears prefer. Furthermore, while we understand some of why this is, some of this gap remains unexplained. In the world of diagnosis, it’s the gap between one that’s serviceable, and one that allows perfect understanding. In the commercial world of Hi-Fi, bridging that gap is what costs so much. Digital and analogue are alternative approaches to Hi-Fi nirvana, just as diagnosis and formulation are to the psychiatric equivalent. Before we get into the nuts and bolts of the alternatives, we need to understand that bias, reliability and validity impact on Hi-Fi as much as they do psychiatry.
Despite the tendency of Hi-Fi companies to stick “Research” in their names, the science of electronic music reproduction, be it analogue or digital, is fully understood. However, when we listen to music, there is so much more happening than modulated pressure waves in the air hitting our ears. Our ears do not simply transfer the sounds they receive to our nervous system: instead, like our eyes, they sample and reconstruct. We are more sensitive to sounds inside the range of human speech than outside; rhythm engages us emotionally, and other cues, such as echo, interference and binary hearing lead to different kinds of understanding e.g., spatial awareness. Our emotional responses to music are also influenced by some distortions e.g., a subtle emphasis placed on high frequencies makes music sound “brighter”, and while the addition of some additional harmonics is experienced as harshly discordant, others are experienced as enhancing. From the perspective of the Hi-Fi engineer, there is thus a constant tension between providing accurate sound reproduction, and introducing subtle tweaks that can simulate the sense of emotional immediacy which comes from the social cues and anticipation associated with a live performance. The Hi-Fi engineer is thus seeking what we will consider “the best” rather than “the correct” reproduction. Because “the best” involves our emotions, which signal our values to ourselves, some of us are willing to spend huge sums to get the value we seek. So, the engineer introduces some distortions to bias the output, which is insufficient to invalidate the connection between the reproduced music and the true original, while also reliably reproducing the emotion we anticipate from our imagined original.
The diagnostician has a very similar task to the Hi-Fi engineer, though the science of diagnosis is much less complete than that of music reproduction. A diagnosis must be serviceable i.e., it should point to effective treatments, if available, and indicate a prognosis. However, the purpose of both treatment and prognosis is to increase the value in our lives, either by removing or adapting to the condition the diagnosis denotes. Thus, in exact parallel to Hi-Fi, there is a tension between description and utility, and because it involves values, people can (and do) make enormous investments in their choices here.
The analogue and digital modes of music reproduction represent two, radically different solutions to the same problem; how to store the information encoded in sound. They’re both shown in the image below
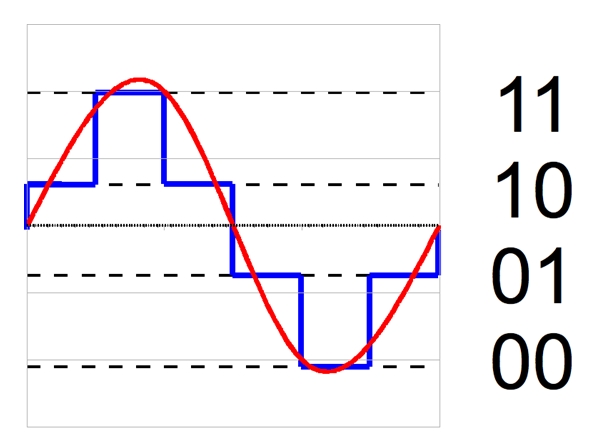
The red, smooth line shows a perfect, visual analogue transcription of a single tone (a sine wave). The blue staircase is a digital attempt to code it, using only two bits, giving four steps in total. These are shown to the right of the figure. The digital coding looks pretty rubbish, doesn’t it? However, that’s because only two bits were used, and there is no limit to the number of bits that can be used. If you look closely at the red line, you’ll notice its edges seem a little blurred, compared to those of the blue one. Look more closely, and you’ll discover that the red line is also a digital staircase, the blurred edges resolving into tiny steps with enough magnification. Thus, digital offers a “gradus ad parnassum” approach to perfection; able to get as close as one likes, but theoretically never reaching it.
Purely analogue reproduction (e.g., vinyl recordings), on the other hand, suffers from a “Garden of Eden” problem
In theory, there are no losses or distortions associated with analogue reproduction. However, this ideal state never survives contact with the real world, and the serpents that live therein. Materials have impurities in them; there is no tolerance without a margin of error, and there are plenty of opportunities for all sorts of added noise to creep into the system. Formal measurement usually confirms that digital approaches provide more accurate reproduction than the best analogue systems. However, analogue systems have never completely died out, and their popularity is now increasing again. Curiously, while quantitatively greater, the biases introduced by analogue systems do not disrupt, and may even enhance, our musical enjoyment, which seems not to be true for digital systems.
It’s hopefully becoming clear that I liken diagnosis to digital, and formulation to analogue methods of sound reproduction. In fact, the earliest system of diagnosis was a 2-bit system. The Smith Papyrus, written by Imhotep in the 17th Century BCE, defines 1) ailments I can treat; 2) ailments I may fight with (though not necessarily win) and 3) ailments not to be treated. Not having an ailment forms the (implicit) fourth step. Here’s an example of how it recommended its diagnoses be employed: the principle hasn’t changed much in around 3,700 years

Of course, many more diagnoses have been developed since then, ICD and DSM being the depositories for those that are most widely accepted in mental health. Keeping our “gradus ad parnassum” analogy going, modern diagnoses are like digital staircases attempting to approximate a smooth incline: dependent on the resolution we seek, we can either say that our approximation is sufficient for our purposes, or insufficient, in which case we need to change our steps accordingly, knowing that while we will never reach absolute perfection, we may be able to get close enough for it to make no difference. In fact, the argument we’ve developed has shown that a “perfect” diagnosis is actually a chimaera. What we’re after is the “best” diagnosis: something that simultaneously denotes the condition sufficiently accurately, while flagging up effective treatments and reliable prognoses which may be worked with, or adapted to. The technical term for this is predictive validity.
Let’s now turn to formulation, the psychiatric (or, in this context, psychological) equivalent of the analogue approach. In theory it should be a perfect model, expressed in words of equivalent meaning and value to all who use it, of everything relevant to the condition and the person experiencing it. This is definitely Garden of Eden territory, given the current state of our knowledge. In particular, the brain, whose functioning seems best expressed by complex mathematical simulations, tends to get left on the “too hard” pile when formulations are constructed, thus excluding the organ we use to experience our mental health. Expressed like this, the formulation seems a futile attempt to erect a pavilion of understanding upon an ocean of ignorance. However, the effectiveness of formulation in delivering understanding on minimal data has long been understood in the arts. Here’s a photograph of the damage done to Guernica

and here’s Picasso’s famous visual formulation of the same event

While the photograph is probably sufficient to determine that something bad had happened, communicating the dreadful truth of mass bombing on unprepared towns required, not more data, but more imagination. Picasso’s Guernica works because verisimilitude has been tempered with Picasso’s emotions, signalling the values we should apply.
Unfortunately, it’s often possible to make opposing formulations about the same states of affairs. Here’s what the Spanish fascists were saying

so it therefore should come as no surprise that psychiatric (or psychological) formulations show much greater propensity to bias, demonstrated through reduced reliability and validity compared to diagnoses. At their worst, they can simply be sales pitches or propaganda, because the information they provide really comes from the storyteller’s understanding, which stands between us and the facts themselves. However, as previously, in psychiatric diagnosis we are after the “best” formulation, so our imagination should be limited to stories which have the closest possible link to the circumstances before us, not the circumstances we would like to believe. This constrains the best formulation to be consistent with the best available science about the circumstances it is attempting to explain.
It’s instructive to see how the Hi-Fi industry has approached its two, very different approaches to music reproduction. There are both digital and analogue purists: the systems either design produce great sound, differing in character but of very similar value. However, whichever you choose, the costs for a top-end system will be eye-watering, and the systems remarkably temperamental (especially if you have gone the analogue route). Ordinary mortals need a different strategy. We cherry-pick our systems across different manufacturers, trying to select components whose strengths support each other, and whose weaknesses cancel each other out. Digital and analogue components thus frequently end up in the same system. Does this approach work? The short answer is yes, with significant cost savings and no appreciable overall loss of sound quality.
In psychiatry, the everyday reality is that formulations and diagnoses are used side-by-side, either explicitly or implicitly. Diagnosis keeps us rooted in our data and evidence. Formulation lets us co-construct imaginative stories that link the science to experience and value, offering both understanding and credible ways forward. Purists continue to try for a “one size fits all” approach, but, just like the hi-fi purists, set themselves tasks which can only be achieved expensively, intermittently and with difficulty, if at all.

Pingback: If diagnosis is so good, why do so many people hate it? | Psychobabel